 |
||
 M6 Cervical vs ProDisc
M6 Cervical vs ProDisc
|
||
|
|
|
|||||||
| iSpine Discuss M6 Cervical vs ProDisc in the Main forums forums; Ok here is my situation last night I was in the YMCA and I seen a friend of mine that ... |
 |
|
|
LinkBack | Thread Tools | Display Modes |
 10-14-2009, 01:03 AM
10-14-2009, 01:03 AM
|
||||
|
||||
|
Ok here is my situation last night I was in the YMCA and I seen a friend of mine that played on my High School Basketball team...He told me that he had a 2 level ADR surgery done in May here in Delaware using the ProDisc at c5-6 and c6-7...Now mind you I was shocked to here that because out of all the doctors I been to in this area none ever mentioned that they could do a 2 level here in the USA...The doctor that is supposedly the best Nero in Delaware even told me he does NOT do 2 levels and that maybe he could do a Prestige at my C4-5 and a Fusion at my C5-6...So I just got of the phone with my friend that got the 2 level ProDisc and he told me the name of the doctor that did the Surgery... So I looked him up and to my suprise he was in my insurance plan...I plan to call him and make an appointment...Here is the thing I need advice on, last week my mom helped me send my MRI and X-Rays to Stenum in Germany because we had been reading alot about the M6 spinal kinetics being the best in the world at this time...I would hate to have my family pay out of pocket to go to Germany unless the shock absorption from the M6 would really make a huge difference in my life...
Thank you to everybody that takes the time to reads this...
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left. 
|
|
10-14-2009, 02:22 PM
|
|||
|
|||
|
Before you jump into the world of ADR or Fusion have you consulted with a neurosurgeon to see if there is a minimally invasive procedure such a a foraminotomy that can help you at least at one level if not both?
As for which ADR is better, it's probably not as much of an issue as opposed to who puts them in. If you have a US surgeon who can do the surgery and get insurance approval, you should really consider staying in the US. Easier follow up care and it seems you have a good reference with you friend.
|
|
10-24-2009, 05:01 PM
|
|||
|
|||
|
Note to those considering older ball in socket designs which can get a bit out of control in multi-level cases, consider the M6 implant, it appears the new designs will have controled motion to help with this. I am looking at Stenum Hospital for 2-3 levels.
|
|
10-25-2009, 09:31 PM
|
||||
|
||||
|
^ Joe56 do you know anyone who has the M6 implant...
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
10-26-2009, 05:42 AM
|
||||
|
||||
|
Joe, I disagree with the concept that the M6 provides stability that is not present with the ball and socket style ADR's. I presume that the theory is that the woven 'annulus' provides additional help here. I've seen the M6 and it's a very interesting design. In theory, I do like what the pseudo annulus does... presumably providing some dampening of the motion at the ADR levels. However, I do not see this helping the 'out of control' concept of multi-level ADR.
The M6 is a mobile core device and, in practice, I see it having the same problem as other mobile core devices. If something provides some off-kilter loading, the core gets pushed to one side and it stays there. Search this forum for the word tiddly-winks and you'll find what I've written about mobile core devices. I have seen several M6 configurations that have this problem. It is a problem in single-level cases too but gets exaggerated in multi-level cases, especially if there is incorrect placement. (I have 3 clients who have had m6's explanted and know more.) The ball and socket designs that have mobile cores (including the M6) will have this problem more than the stationary core designs. Having said that, I spoke to a friend tonight. He is the first patient in the world with a 4-level Mobi-C (highly mobile core) and is several years post-op with no stability issues at all. I'm going to COPY the M6 posts to the M6 vs. ProDisc thread (M6 Cervical vs ProDisc) that was started a few days ago. This thread is very long and involved and devoted to Steve's ordeal. All the best. Mark
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org
|
|
10-26-2009, 05:53 AM
|
||||
|
||||
|
I just copied the 3 previous posts from another thread. (I didn't want the M6 discussion to get buried in a very long thread about something else.)
To continue, the soft core of the M6 does promise to provide some shock absorption. Intuitively, that seems to be a great idea. We do have 22 shock absorbers in our spine and it remains to be proven how important getting some cushion at the ADR levels will be. I expect that it will be like most of the other features we see with all the devices... there will be some advantage, and some disadvantage. Will it break down faster? Will it change shape? Wear particles and their effects? I don't know the answers to these questions. It's tough to sort out the marketing spin from the important features. The keeled devices keep the prosthesis from rotating, but if the cleated devices don't rotate, how important is that? There are advantages and disadvantges to keels and cleats, but my point is, the discussion about arresting rotational forces is not relevant to us as patients... but it's effective marketing. Mark
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org
|
|
10-27-2009, 02:52 AM
|
||||
|
||||
|
Quote:
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
10-27-2009, 09:30 AM
|
||||
|
||||
|
JKDE302,
The 3 posts above were originally on steve's 'tilted all over the place' thread. I left them there, but copied them to this thread. Mark
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org
|
|
10-28-2009, 02:23 AM
|
||||
|
||||
|
So if there are stability issues with multi-levels, why are the surgeons not doing more hybrids, the combination of fusions and ADR? That way the top level will have the mobility that seems so necessary to prevent adjacent disc disease, but the fusion below provides stability.
I just found out that the m6 is the only disc on the market that I am not allergic to, so I'm trying to sort out where and how to get it without losing my home.
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium.
|
|
10-29-2009, 12:53 AM
|
||||
|
||||
|
Quote:
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
10-29-2009, 07:41 AM
|
||||
|
||||
|
Because it is the only one on the market I've found that does not contain cobalt, chromium or nickel, to which I am highly allergic. It is made of surgical grade titanium, and then covered with 100% titanium.
I had a blood test at Rush University with gave me the list of different metals to which I am intolerant. I knew I had a problem with nickel because of skin allergies with jewellery my whole life, but this test confirmed that I have a much broader problem than just nickel. Titanium is the only metal that I can safely tolerate. It literally saved my life by preventing me from having to go through a five level revision surgery.
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium.
|
|
10-29-2009, 03:35 PM
|
||||
|
||||
|
^ I wonder what my body is allergic to also should I get a test done?
Am I wrong for thinking the M6 would be more secure b/c of the extra keels and I will need the shock absorption to start off my 30's?  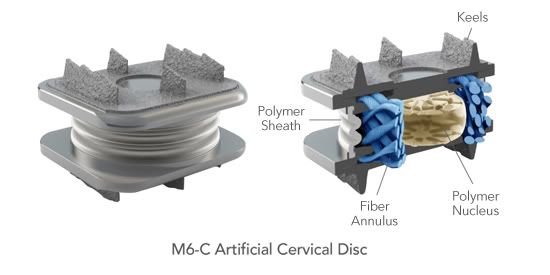
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
10-29-2009, 06:51 PM
|
||||
|
||||
|
Do you have any symptoms of metal allergies, or other allergies for that matter? I can't wear most jewellery, and I have recently developed a multitude of food and drug allergies. So when someone on a forum suggested that I have this metal allergy test done, I decided it was money well spent.
The surgeon who was supposed to put in several Maverick discs last week had a change of heart, and now I have to figure out how to get the M6 without losing everything I own. The surgery last week would have been covered by insurance. Now...I really don't know what is going to happen. It isn't available here yet because of regulations. If you feel that you want to have the allergy testing, just as insurance, you can PM me for details, or just contact Rush University in Chicago. I have heard of one other patient who had no previous symptoms and still had reactions to an implant. But it isn't hard and fast, just another person's story. My surgeon did tell me about a conference he was at last May, and there were reports of four spine patients who had revision surgery because of metal allergies. That's why he was so careful about my nickel allergy. While the test isn't cheap, it certainly beat the alternative. Now I have no other options; I have to have the M6, no matter what the pros and cons are. I am considering asking for fusion at the bottom level, then the two artificial discs above that in the lumbar, to reduce the excess movement that has been brought up. But I guess the final decision is the in the hands of the surgeon, whoever that may be.
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium. Last edited by Katie; 10-29-2009 at 06:53 PM.
|
|
10-29-2009, 08:25 PM
|
||||
|
||||
|
Katie, Bryan and Prestige LP are titanium. Newer prestige is titanium and ceramic.
JKDE302, more secure only matters if less secure is a problem. I don't think that more smaller keels are necessarily more secure... it will likely depend upon how much surface area interfaces with the bone. We talk about primary and secondary fixation. Primary fixation is the 'stay puttedness' of the device upon implantation. Secondary fixation occurs after osteointegration of bone and the coating on the prosthesis. After osteointegration, migration is unlikely even in the 'no keel, no cleats' design (PCM). PCM has a double whammy of poor primary fixation AND the large radius joint surface that does not keep everything centered. I believe that the clinical trials were halted because of migration. (This is what I was told by a surgeon in the trial. I do not have any documentation about this.... I consider it a rumor, but because of the source, I trust it.) Migration or expulsion of the prosthesis has been seen in all devices, but I've never seen it ever, ever, ever; with properly implanted devices. I'd rather have a well placed PCM than a poorly placed ProDisc or other device... even though the device factors should be discussed, understood and considered... IMHO, the choice of surgeon is far more important. Mark
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org
|
|
10-30-2009, 03:28 AM
|
||||
|
||||
|
I could not get accurate, specific details on the purity of the titanium in either of these discs.
Can you tell me EXACTLY what titanium alloy is used in them? And are they covered with a 100% titanium spray?
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium.
|
|
10-31-2009, 08:50 PM
|
|||
|
|||
|
Mark,
I understand your concerns. What I have learned is that the Spinal Kinetics guys studied the physical characteristics of the human disc and placed these parameters into their test computers, then they began the process of prototyping an implant that replicated these characteristics. The result was a disc that might just be the first to actually deserve the name artificial disc. The goal of course is to return the spine to normal function. Now we both know that as the damage from years of degeneration progresses the other structures and tissues become unable to respond normally. The selection of candidates is critical. Surgeon placement errors and patients whose bodies just cant keep the implants in place will always come up, but overall I think the goal of returning to a normal function is attractive. Others, Stenum tells me the new insertion process used with M6 means less time in the OR, less blood loss, and seems to have improved the "Primary fixation or the 'stay puttedness' of the device upon implantation" as Mark states. Joe
|
|
11-03-2009, 02:32 PM
|
||||
|
||||
|
Mark, I checked out the Bryan website and it said that it is approved for single use only. I have three levels in my lumbar and two in my cervical that need work.
What information do you have about the metal content of either of these? Unfortunately there is nothing on their site about that. I'll try calling them again to see if I can get an answer.
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium.
|
|
11-06-2009, 03:33 AM
|
||||
|
||||
|
I dont have money to go to Stenum so i guess this thread was a waste of time unless it helped somone else..Idk maybe i can wait to get in a US trial for the M6 maybe I cant..Im so dissapointed to think they make disc with shock absorption and I just turned 30 and cant get one...Im feelin near suicidal right now, I hate this fuchin world....Fuch the FDA...
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
11-06-2009, 03:22 PM
|
||||
|
||||
|
You're in very good company, my friend. I've been trying for almost two years to get to Stenum for four levels. Now it has grown to five. I've been battling the insurance gods, which in my case is our Provincial Government.
Then I finally found a surgeon in another province who could do the surgery and be covered, free of charge, but then this allergy issue came up. So what I can tell you right now is to take the time to rant, scream, kick (but don't hurt  ), just anything to get this legitimate anger out of your system. It may take a week or a month, but don't let depression take its place. ), just anything to get this legitimate anger out of your system. It may take a week or a month, but don't let depression take its place.Then start again on your search for something that works. I've found out that there are a number of trials both on now and upcoming. Unfortunately they won't work for me, but you can google trials for spine surgeries, etc. Age is a relative thing. While I'm a fair bit older, I had just started life again when this hit almost five years ago. I had just met and married the love of my life and was looking forward to enjoying everything that I never had, travel, adventure, a new job...now it is all on hold until this is resolved. You have a big advantage over me. Even if you decide to use one of the other discs and they deteriorate after ten, fifteen or twenty years, just think of the new technology that will be out there, and may replace what you might get now. And you'll still just be coming up to the age I am now. Believe me, 50+ is not old , not when you are there. And you will still be in the age group that they will consider working on. Me, I'll be way over the hill if something breaks...I'll be toast. So yes, rant for awhile, but then start again!!!! You said it yourself, you have your whole life ahead of you, so make plans to enjoy it. Take that brilliant young brain of yours and put it to use by investigating every option out there. Believe me, they are there. Any chance of anyone taking money out of retirement funds or taking a loan? Those are some options others have used. And I know the frustration of not being able to do those either. It took me two years to get a diagnosis and finally find someone to prescribe some pain medication. Then almost two more years of battling the insurance and now that plus the allergies, but I am not quitting. Every day feels like I am getting closer to the solution. Did I feel like quitting both for the day and forever? You bet. More than once. But I long ago decided to not let the bas*@*ds win. They Will Not Win. Check out the Insurance Warrier's website. She has some very good ideas about battling insurance companies, if you need that now or later. If you ever want to just rant some more, or toss over some ideas, feel free to PM. I'm here, and will continue to be even if (no, when) I win this battle. Good luck. And no post like this is ever useless....
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium.
|
|
11-06-2009, 03:39 PM
|
||||
|
||||
|
Mark, thanks for the suggestion about the other discs being Titanium. Unfortunately they are made of surgical grade Titanium, which is a 6/4 alloy, meaning that they also include 6% Aluminum and 4% Vanadium.
I am highly allergic to Aluminum, so unless they will custom make me a disc that is covered in 100% pure Titanium over top of the 6/4 alloy, it might as well be made of Nickel. While science was never my strong point, I am fast learning the finer points of chemistry and physics because of this.  I have spent the last week investigating all of this and speaking to the engineers at a great number of spine hardware manufacturers. These are some of the top guys in the world, and they are happy to spend time talking to me, I assume because of the uniqueness of my case. Several have suggested that I go through the sales reps for my surgeon and have them ask their companies about making a custom appliance, so that's where we are going next. I'm not meaning to hijack this thread, but add to it by showing that there are ways around everything. I was so discouraged at the beginning, after being turned away from several options. It turns out it was literally a life saver. If I had gotten what I wanted right away, I would have been full of hardware made of cobalt, chromium, nickel, just about everything that I am highly reactive to. I can't imagine how ill I would be, or if I would even be alive right now. So my point is, be careful what you ask for...you just might get it, and it may not be the best thing for you at the time. If you come across any surgeons, anyone who can guide me to an alternative to surgical grade titanium or any of the other metals, I'd really appreciate it. Thanks. Edited to add: the M6 apparently does not have pure Titanium coating over the sides of the metal, only on the endplates. I have to double check as I understood it to be different, so it may not work for me either.
__________________
DDD Herniated discs C4/5 & 5/6, L3/4, L4/5, L5/S1 Severe compression of spinal cord in two levels All conventional therapy exhausted, including spinal injections, PT, massage, etc. In appeal with Gov't Insurance for Out-of-country coverage for ADR hybrid surgery of above discs. Recently discovered that I am severely allergic to all common metals used in surgical hardware except for Titanium. Last edited by Katie; 11-06-2009 at 03:42 PM.
|
|
11-06-2009, 03:45 PM
|
|||
|
|||
|
JKDE,
I was 28 when I injured my spine back in '82. The spinal technology back then was much less than it is today and believe me I know I suffered the consequences as have many others with just shear availability/options. I too waited for the FDA to approve of multi-level lumbar disc replacement so WC would pay for that vs. fusion and ADR (with Prodisc) but now I have more DDD while waiting, facet degeneration at L4 and L5S1 and my L5S1 has finally autofused which I think is the best thing about the prolonged course of my "doing nothing more/waiting and seeing" and so forth. Your feelings are quite understood here. Yet I think you are in a good position if there is a good option out there available to you and your insurance company covers it. Meanwhile keep researching as Katie mentioned. I don't mean to "mother you" but I am 25 years older than you and have been down a spinal road of "waiting and seeing" and doing nothing more surgically for various reasons some of that waiting for things to be FDA approved that have just been taking FOREVER.. You are young and you do have a lifetime ahead of you so hang in there and keep going. That being said I certainly understand how you feel and have been there in the past myself. Keep going. You're in good position just being young!!!
|
|
11-06-2009, 04:30 PM
|
||||
|
||||
|
JKDE,
There is now an elephant sitting in the middle of your living room and, however unpleasant, it needs to be addressed. Death is a permanant solution to a temporary problem. While some diseases worsen over time and are not a temporary problem, your spinal problems are not among them. What you do have is a money problem and though it may seem permanant, no one has a crystal ball as to what might be just around the corner. Having been there, I understand your anger. I was fortunate to be living in California and tapped into the equity of our home to go to Germany. You might think it's easy for me to sit in judgement of your problems because I already got my 'miracle' but I once sat for five years thinking there was no solution. A four level fusion was and is contra-indicated and I had never even heard of any artificial disc replacement. When I started my journey, they had not yet been FDA approved for a single level let alone a multi-level. I saw no way out of my constant pain or living as an invalid. BUT, life's difficulties have taught me that down doesn't last forever. As more discs pass FDA trials and longevity factors replace speculation, the insurance companies will have to eventually recognize the value of these motion preserving devices. I believe this is just around the corner. BUT, when broken down, you still only have financial difficulties. The only thing between you and your solution is money. There may be those who feel money is the only thing worth living for but they don't travel in my circles and I suspect not in yours either. I would also like to point out though not the best solution or the one you want, fusion is also a possibility. I'm not suggesting you give up the fight or your anger but it is another way to go to end your pain and suffering. One more thing - however difficult, find something to laugh at - a joke, trying to get dressed, someone elses stupidity like the woman who phoned 911 to report herself as a drunk driver ") . . Most of life's wonderful moments are ahead of you. Wouldn't you like to be here to enjoy them? You are in my thoughts, Dale
__________________
3 level Prodisc adr S1-L3, Oct 12, 2005 Dr. B in Bogen, Germany Severe nerve damage in left leg, still working on it
|
|
11-06-2009, 08:31 PM
|
|||
|
|||
|
JKD,
Are you only interested in the M6? Have you tried to get insurance coverage for a ADR in the States? It may not be an M6 but their are "battle proven" ADR's. Also Fusion is not a "death" sentence by any means. I had one and played basketball, Tennis, work out and even road roller coasters (don't tell the DR.). Hope is not lost, just a different fork in the road.
|
|
11-07-2009, 10:42 AM
|
||||
|
||||
|
Thanks for the support everyone....I really mean that....
I think it just makes me sad that I need surgery asap and cant wait this out, I coach high school basketball at a super competive public school and really think my spine will need that "shock absorption" to continue my life...I almost wish i never heard of the M6 now..If it was (Not) for all the vicodin and marijuana in my system to help keep "my cool".. I would probally be starring into the eyes of a nervous bank teller with one of (those things) in my hand saying "I dont want to harm you but I really need this money right now"... Obviously it would not be comfortable on my neck in prison.. I have not reached that level of insanity yet but i can only wonder what the future will hold for my state of mind.. I have alot of respect for the resilience of all of you who have spine problems.. I use to laugh at my old injuries like complete knee tears of ALC, MCL and both meniscus...Broken ankle in multiple places ect..Spine problems are literally "on another level"... Note: I can see how people could lose their mind and commit random acts of violence, And from another perspective I could only imagine that the people who turn to suicide do it because they feel sleeping is better then being awake... dshobbies: the woman who phoned 911 to report herself as a drunk driver was beyond hilarious and brought a smile to my face for at least 90 seconds...lol .
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left. Last edited by JKDE302; 11-07-2009 at 10:55 AM.
|
|
11-08-2009, 12:17 AM
|
||||
|
||||
|
^ I left that post during a negative thought process, I apologize...Today I did yard work and pulled loose vines sticker bushes...the pricks in my skin from the sticker bushes took the pain away from my neck...I wouldnt mind if I got just a little poison ivy if it takes my focus off my spine...
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
11-08-2009, 09:21 PM
|
||||
|
||||
|
JKDE,
One thing around here is that most of us have probably walked in those dark shoes a time or two ourselves and we understand. No need to apologize. It's during those times that you should post and allow us to help. It's important to know that others survived those feelings and have come out the other end. I was going to say we came out whole but whole has a new definition for most of us too. I still have my down days but those dark ones are gone. With any luck, you'll be posting the same soon. I do hope so! Dale
__________________
3 level Prodisc adr S1-L3, Oct 12, 2005 Dr. B in Bogen, Germany Severe nerve damage in left leg, still working on it
|
|
11-18-2009, 10:42 AM
|
||||
|
||||
|
Thanks Dale... I want to be done with the dark days also...
__________________
C4-5: Mild disc height loss with central annular fissure. Small broad-based left paracentral disc protrusion. Moderate central canal stenosis-the disc protrusion abuts and mildly flattens the left ventral surface of the spinal canal. C5-6: Disc desiccation with mild height loss.Diffuse discosteophyte bulge and uncovertebral joint hypertrophy, moderate central canal stenosis- Severe neuroforaminal stenosis bilaterally, right greater than left.
|
|
| Bookmarks |
|
|






 Linear Mode
Linear Mode



